

Navigating our Public health System. Part 2 - Worker’s Compensation and Motor Vehicle Accidents.
Dealing with injuries from work or a car accident are already stressful enough without trying to get your head around managing who's paying for what, which forms you need, and who you're even supposed to be calling. It's a lot to juggle on top of recovering.
If you've ever been injured at work, or been in a car accident, you'll know the injury is often only half the battle. The other half is figuring out who's paying for what, which forms you need, and who you're even supposed to be calling. It's a lot to juggle on top of recovering.
In Part 1, we walked through Medicare, subsidised scans, and DVA. In Part 2, we're covering the two other funding pathways we see most often at Formotion Physio:
Workers' Compensation and Motor Vehicle Accident (MVA) insurance through ICWA. Both can cover your physiotherapy with little to no out-of-pocket cost once your claim is accepted, but getting there involves a slightly different process to a standard Medicare or private appointment.
Please note all advice below is general in nature and subject to change. Rates, forms and processes are set by WorkCover WA and the Insurance Commission of Western Australia (ICWA) and can be updated at any time, so always confirm current details directly with your insurer or case manager.
Glossary
Before we get into it, a couple of terms worth knowing:
Claim Number - the reference number your insurer gives you once your claim has been lodged. You'll need this before we can bill your insurer directly. If you don’t have one yet you can still access treatment and potentially claim it back later once the claim has been accepted.
Case Manager – the person at your insurer who oversees your claim, approves treatment, and is your main point of contact for anything claim-related.
Rehab Provider - a person / company who accepts as a liaison between everyone involved: You, your employer, your case manager and any other health providers like your GP or Physio. Not everyone is assigned one.
Part 2a. Workers' Compensation
What is Workers' Compensation?
If you're injured at work, or your condition arises out of your employment, your employer is required to hold workers' compensation insurance to cover the cost of your treatment (and, in many cases, a portion of lost income while you recover). In WA, this scheme is regulated by WorkCover WA, though the actual claim sits with your employer's insurer.
How Do I Access Physiotherapy Under Workers' Compensation?
The process looks a little different to booking a standard appointment:
Report the injury to your employer as soon as possible, so they can lodge a claim with their insurer.
Once lodged, you'll be issued a claim acceptance letter and a claim number – you'll also usually be assigned a case manager.
You'll need a GP referral to start physiotherapy under your claim.
When you book with us, bring along your claim number, claim acceptance letter, and your case manager's name and contact details (you can also select "Workers' Compensation / Motor Vehicle Accident – New Assessment" when booking online).
From there, we liaise directly with your case manager to get your treatment plan approved at WorkCover WA rates. Once approved, we bill the insurer directly, so there's no out-of-pocket cost to you for treatment covered under the plan.
If your paperwork isn't sorted yet but you don't want to delay treatment, you can pay privately in the meantime and potentially claim the cost back once your claim is accepted.
Key Points:
A GP referral, claim number and claim acceptance letter are needed before we can bill your insurer directly.
Once your treatment plan is approved, there's generally no out-of-pocket cost for covered sessions.
You can choose your own physiotherapist under Workers' Compensation – if you'd like to switch providers, just raise it with your case manager.
Missed appointments and late cancellations aren't covered by WorkCover WA, so those fees remain your responsibility.
Part 2b. Motor Vehicle Accident Insurance (ICWA)
What is ICWA Motor Injury Insurance?
If you're injured in a crash caused (fully or partly) by someone else's driving, cover generally comes through the Insurance Commission of Western Australia (ICWA), which administers the compulsory third-party motor injury insurance built into every WA vehicle registration. It's not just for drivers – passengers, pedestrians and cyclists injured by a vehicle can also be covered.
How Do I Access Physiotherapy After a Car Accident?
Report the crash (via crashreport.com.au if applicable) and lodge an injury claim with ICWA.
Once your claim is accepted, you'll receive a claim number – this is what allows us to bill ICWA directly for your sessions.
A GP referral isn't strictly mandatory for an ICWA claim (unlike Workers' Compensation), but we'd still recommend one, so we can liaise with your GP where needed.
As with Workers' Compensation, you can book online under "Workers' Compensation / Motor Vehicle Accident – New Assessment."
If you don't yet have a claim number when you're ready to start treatment, sessions can be paid for upfront, with the possibility of claiming the cost back once your claim is accepted. How long that acceptance takes varies quite a bit from case to case, so it's worth chasing your claim status directly with ICWA if you're unsure.
What Does ICWA Cover?
ICWA can cover a broad range of "reasonable and necessary" treatment, including ambulance, hospital and medical costs, imaging, medication, and allied health services such as physiotherapy. Fees are paid up to maximum amounts set out in ICWA's published fee schedule (benchmarked against AMA and WorkCover WA rates) – so most sessions are covered in full, though a gap may apply if a provider's fee sits above the scheduled maximum.
Common injuries we see from motor vehicle accidents include whiplash, concussion, and knee, hip or other joint injuries from impact or high-speed collisions.
Catastrophic Injuries Support
For the small number of people who sustain very severe, life-changing injuries in a crash – regardless of who was at fault – ICWA also runs a Catastrophic Injuries Support program, providing longer-term treatment and care funding outside the standard claims process. If this applies to you or a family member, it's worth asking your case manager or contacting ICWA directly for details, as the support pathway differs from a standard injury claim.
For more info on ICWA and Motor Vehicle Accidents vist: https://www.icwa.wa.gov.au/motor-injury-insurance/make-an-injury-claim
Key Points:
You'll need an accepted claim and claim number from ICWA before we can bill them directly.
A GP referral isn't mandatory, but we recommend one so we can coordinate your care.
Most reasonable and necessary treatment is covered up to ICWA's fee schedule maximums – ask us if you're ever unsure whether a gap will apply.
Severely injured? Ask about ICWA's Catastrophic Injuries Support program.
In Summary
Both Workers' Compensation and ICWA claims can fund your physiotherapy with little to no cost to you once accepted – the main things to sort out early are your claim number, claim acceptance, and (for Workers' Compensation) your GP referral. If you're not sure where your claim stands, our admin team is always happy to help you figure out next steps.
To book a Physiotherapy consultation at either of our locations in Osborne Park or Joondalup, click the button below:

Navigating our Public health System. Part 1 - Medicare and Physiotherapy.
Part 1 of this blog gives an overview of Medicare in the context of Physiotherapy conditions and how you may be able to use it for Physiotherapy and associated scans like X-Rays, Ultrasounds and MRIs.
In the midst of the stress and pain of an injury, the last thing you want to be doing is figuring out how our health system works and how you might be able to access funding, public or private, to pay for your Physiotherapy or associated costs.
This blog is to give you an overview of how you may be able to access funding in the context of accessing Physiotherapy in a private practice.
Please note all advice is general and subject to change, and we would advise you to look into each funding body in more detail if the time comes that you need it!
Part 1. Medicare funded or subsidised healthcare.
Medicare subsidised Physiotherapy (CDM)
Medicare subsidised scans: X-Rays, Ultrasounds, MRIS, CT Scans.
Emergency Department (ED) vs St John’s Urgent Care
Department of Veterans Affairs (DVA)
Glossary:
”Rebate” - A partial payment or refund, you either pay the full amount up front to the practice and are then refunded a portion after an appointment, or the fund pays a portion directly to the practice and you pay the “gap”.
“Bulk Bill" - You don’t pay anything and the insurer / fund pays the practice instead.
Medicare funded Physiotherapy sessions
What is Medicare?
Medicare is Australia’s universal health insurance scheme. Australians help to pay for Medicare from income tax. How much you pay depends on your income.
What does Medicare fund when it comes to private Physiotherapy practices?
If you have a chronic condition, or complex care needs that are overseen by a GP, you may be eligible to receive a referral from your doctor, referred to as a GP Chronic Condition Management Plan, or “GPCCMP” (Previously CDM, and before that “EPC”).
With this you can access 5 Medicare subsidised Allied Health sessions (including Physiotherapy and Exercise Physiology) sessions per calendar year.
The amount Medicare subsidises at time of writing isaround $63.40 (updated July 2026)
While some Physiotherapy clinics may offer “bulk billing”, most clinics will require you to pay a gap as this amount does not cover the costs of a standard appointment.
An important point to note is that these sessions are counted in each calendar year, so it’s best to try use your sessions within the year as the number is reset at the start of each year.
For example, if you received your GPCCMP referral for 5 sessions in November 2026, but only get to 3 appointments, the leftover 2 sessions are counted towards your 5 sessions in 2027.
For more information visit this link
2. Medicare funded or subsidised scans
Medicare funds a portion of certain scans like X-Rays, Ultrasounds (US) and MRIs that you may need to help investigate certain diagnoses.
X-Rays and US are generally cheaper and can be good as an initial investigation to investigate boney tisue and soft tissue respectively.
MRIs can provide a lot more information on conditions and can visualise larger areas in more detail including soft tissues, joints, bones, muscles, or cartilage and may show things that may be missed on X-Ray and US.
They are however quite expensive and generally cost $300+ depending on the radiological company. Some of the common ones are SKG, PRC, I-Med and Envision.
For Medicare cover it is often required that these scans are referred by a specialist doctor for them to be covered, either partially or fully. There are a few conditions / areas of the body that your GP can refer you for that will get you the medicare rebate, but we would recommend talking to them for the most up to date advice on this.
Key Points:
Physiotherapists can refer for Xrays, Ultrasounds and MRIs - however some Xrays, Ultrasounds and all MRIs are not rebatable by medicare if referred through Physio. This means we can give you a referral but you may pay more out of pocket.
Most X-Rays and Ultrasounds referred by GPs are bulk billable. Some MRI’s are bulk billable but only for certain conditions.
Physiotherapists cannot refer for CT Scans
Medicare will generally give higher rebates for MRIs and many other scans if referred by specialists, Sports Medicine Physicians (Sports Doctors) and Orthopaedic Surgeons. However, their consultation fee in itself may be quite costly, and often you’ll need a referral from a GP to see them as well, particularly Orthopaedic Surgeons.
Often deciding what to do will depend on whether cost or the quickest most direct route is more of the priority. Sort of like booking flights to Europe!
3. Emergency Department (ED) vs St John’s Urgent Care.
St John’s urgent care is a new initiative that has been designed to ease the overwhelm of our Emergency Department. At St John’s Urgent Care you can often be seen much quicker for injuries and conditions of an urgent nature non-life threatening, like bad sprains, breaks or back pain.
Generally if you head to the ED with a non-life threatening condition, especially for musculoskeletal issues, the triage system which decides the priority of your medical condition will put you towards the bottom of the list which means you could have excessively long wait times.
In these instances you may be better off heading to a St John’s Urgent Care where you are likely to receive treatment quicker. You may also be able to receive better advice in what to do in the aftercare, as often this is impossible to do in the Emergency Department when it is very busy.
The conditions that you should head to the ED are generally things like the following:
Chest pain or tightness
Breathing difficulties
Uncontrollable bleeding
Severe burns
Poisoning
Unconsciousness or seizures
Numbness or paralysis
A life-threatening injury
On-going fever in infants
Unresponsive
It is also important to note that regardless of whether you are cleared in the ED or at St John’s Urgent Care for a musculoskeletal injury you should still get it followed up by your GP or with a Physiotherapist for advice on what to do next if there is still treatment or rehab required (like an ankle sprain).
As you know often a full Physiotherapy assessment and treatment plan can take much longer than the 10-15mins you may only get in our emergency departments. While treatment in the ED is often completely covered by Medicare, and subsidised at St John’s Urgent Care often this is reflected by the limited time and individualised care and aftercare you may receive.
4. Department of Veterans Affairs (DVA)
What is DVA?
The Department of Veterans Affairs is a department of the Australian Government and provides certain support, health care and rehabilitation services and information for veterans, their dependants and a range of other associated people. While it is not directly funded by Medicare a lot of the systems are similar which is why we have included it here.
How Do I Access Physiotherapy Services Under DVA?
You may be able to receive physiotherapy services if you have an assessed clinical need and:
a Veteran Gold Card; or
a Veteran White Card and your treatment is for an accepted service-related condition. e.g. Osteitis Pubis
You’ll need a referral from your GP or another medical practitioner. The referral allows you access to 12 sessions and this lasts for 1 year only (then you’ll need another referral).
All sessions under DVA are “bullk billed” meaning you won’t pay anything to your Physiotherapist.
Stay tuned for Part 2 of Navigating our Health System where we will cover:
Worker’s Compensation (WC insurance)
Motor vehicle accident insurance (ICWA)
Private Health Insurance (PHI)
Let us know in the comments if you have any requests or questions.
To book a Physiotherapy consultation at any our locations in Osborne Park or Joondalup click the button below:

3 Metrics You Should Measure as a Distance Runner
If you are constantly battling running injuries, consider measuring these 3 things to see if you are overloading yourself.

Most people only track their pace and distance when measuring their running load. But when it comes managing injury risk, there are better metrics to track!
If you are constantly battling niggly running injuries, try keeping track of at least 1 of these and see if it starts to make a difference.
1. Heart Rate
Most people run too hard, too often. Keeping track of your heart rate during your runs helps manage intensity, fatigue, and recovery so training stress builds fitness without tipping you into overload.
If you only ever train in zone 4 or 5, when you should be in zone 2 or 3, this may be part of what is pushing you into the danger zone of injuries.
2. Cadence
Cadence measures how many steps you take per minute. A lot of beginner runners take too few steps per minute, resulting in overstriding. Small cadence changes can reduce braking forces and joint load, often useful for managing common running injuries.
As a rough guide we generally recommend aiming for about 160 - 180 steps per minute (less if running slower, more if faster). This is by no means a magic bullet, but it can give you a good place to start from.
3. Stride Length
Runners who land with their foot ahead of their centre of mass (overstriding) consistently show higher joint and tissue loads. Reducing your stride length can be a game changer in reducing your risk of injury and improving your running economy.
To check if your stride length is too long you can get a friend to film you side on, if your foot is landing in front of the drop down line from your knee this can often indicate that you are “putting on the breaks” rather than propelling yourself forward, leading to excessive joint force and a loss of efficiency.
Check out this video here to help: https://www.instagram.com/p/BYfGo8nDcrU/?igsh=MTZnczRwa3AxN2V4eQ==
By Mark Rennick - Senior Physio for Runners at Formotion Physio.
Check him out and book in with him here.

The Importance of Strength Training for Older Women
Strength training is not just for men, on the contrary it is one of the most important things you should be doing as an older woman.
Strength training is not just for men.
Strength and balance training is hugely important for women, particularly as you age, from both a physical and mental health perspective.
However, a lot of older women find gyms intimidating and find the thought of lifting weights scary or are held back by the idea of weight and strength training being “not for women”.
On the contrary it absolutely is, for the following reasons, and a whole lot more!
Improves your bone density and reduces risk of osteoporosis
Improves mobility and reduces your falls risk as you age
Improves some menopausal and pelvic floor symptoms
Improves your sleep quality and mood
Improves your cardiovascular health
Can help with weight fluctuations due to hormone changes
Empowers you to do more independently and feel safer within yourself

As you start to reach menopause your levels of oestrogen and other hormones drop. Because oestrogen helps maintain bone density, this drop can lead to significant bone loss and to low bone density over time.
Weight bearing and resistance (strength) training signals to the body to keep regenerating bone which helps to maintain your bone density. It also builds muscle, tendon and ligament strength to support your joints, and lift heavy things on your own!
Improved strength, balance and agility means you are less likely to fall, and also less likely to injure yourself badly if you were to fall. You will also be able to get yourself up off the ground after a fall, which is extremely important particularly if you live alone.
Menopause can also cause an increase in pelvic floor and incontinence symptoms as you begin to lose elasticity of the muscles of the pelvic floor.
Combining pelvic floor exercises with your strength training, and adding in things like small jumps and change of direction movements teaches your pelvic floor how to contract and relax quickly. This can be helpful for situations in life like jumping off a small wall, sneezing or running small distances.
Why you might avoid strength training, even when you know the benefits.
Often it can feel intimidating going into the gym or the weights section. It may feel like lifting weights is just for men or people in their 20s!
While there are many gyms, bootcamps and group exercise classes that are designed for women, we know that sometimes even the thought of starting those without any previous experience, or “knowing what you are doing” can be rather terrifying.
You’re possibly worried about injuring yourself or don’t believe that you can lift the heavy weights.
You’re worried about getting “bulky” or “too muscular”.
You might avoid doing classes because they involve jumping or running, which very often causes stress urinary incontinence (leaking urine).
You might have even been told in the past that lifting weights would damage the pelvic floor. However we now know that with the correct technique and slow progression of weights, you can actually improve your symptoms by strengthening the pelvic floor along with the rest of the body.
How we can help you move beyond these (sometimes literal!) hurdles:
We start off with one-on-one sessions so you will be completely supported and not have to worry about “knowing what to do”.
As Physiotherapists we are experienced with training around pain and injuries and can modify almost anything to allow you to still exercise safely.
As we have extra experience in strength training we are able to help you progress from injury or a low baseline in strength, right up to competence in doing things you probably never realised you were capable of!
You will not get bulky or big with the kind of exercise we’ll be doing, the kind of training needed to build visibly big muscles requires a specific kind of training and diet, repeated for years! You will likely just improve your muscle tone.
We are all trained in pelvic floor rehabilitation and so can incorporate exercises that will improve your function, as well as give you appropriate exercises that won’t stress the pelvic floor beyond your current capabilities.

Does this sound like something you would like help with? Feel free to book an Initial Assessment via our booking page with any of our experienced team.
Click the button below.
Alternatively give us a call on 0422 483 865 or email admin@formotionphysio.com.au
We have locations within gym settings in Osborne Park, West Perth and Joondalup

Concussion Story: Part 2 - By Jess Bell
In Part 2 of this blog, Jess talks about how concussion SHOULD be managed and strategies for recovering from post-concussion symptoms if they arise.
Last blog I shared my own journey with concussion and showed how easy it is to mismanage athletes who have been concussed. Today we take a step forward in the right direction and discuss how to appropriately address concussion.
It’s important for athletes, coaches and support staff to have a clear understanding of concussion and how to manage it. Too many athletes have had their careers - and tragically even their lives – cut short due to poor handling of concussion.
What is concussion?
Before we address concussion management, it’s important to understand what concussion actually is.
Concussion is a traumatic brain injury. Not just a head knock, or getting your bell rung.
A concussion can be caused by a direct blow to the head or rapid deceleration of the head and neck (e.g. whiplash). This force is transferred to the brain, which moves rapidly back and forth in the skull. This causes chemical changes in the brain and can damage brain cells.
These chemical changes are what cause our immediate signs and symptoms. These can include:
Headaches
Dizziness
Neck pain
Difficulty concentrating
Fatigue
Sensitivity to light
Sensitivity to noise
Forgetfulness
Irritability
Sadness
You do not have to lose consciousness to sustain a concussion. The severity of the concussion is not related to whether you experienced loss of consciousness or not.
How do we manage concussion?
When an athlete sustains a concussion (or suspected concussion), they must be removed from the field of play IMMEDIATELY. The first priority is to get medical help, whether at an emergency clinic, a GP or sport doctor. It is the medical team’s role to diagnose a concussion and set the return to play protocol in motion.
The following table provides the stages of concussion management and approximate timeframes. These timeframes are not rigid – athletes must complete 24 hours at the current stage without recurrence of symptoms before progressing to the next stage. If an athlete experiences an increase in symptoms, they must regress to the previous stage for at least 24 hours to allow the brain to recover.
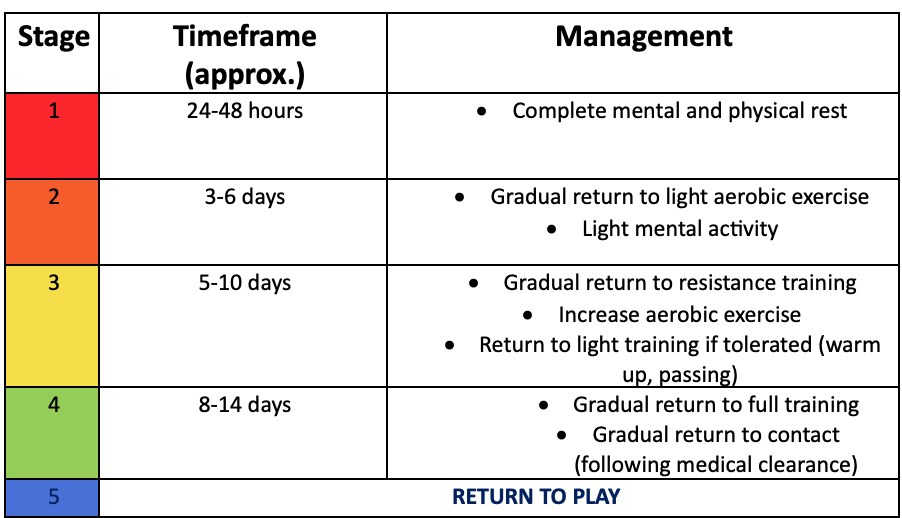
For further information on the concussion return to play protocol, visit https://www.concussioninsport.gov.au/home
It is essential that the medical team (GP, sports doctor, physio) and the support staff (coaches, managers, S&C) have clear communication with the athlete and each other throughout the journey. Collaboration is essential to ensure the athlete has the smoothest and most effective recovery from their concussion.
An athlete must be medically cleared before returning to full training, and again prior to returning to play. No athlete should be allowed to play without a complete formal medical review and clearance. The risks are too great.
What if my symptoms aren’t easing?
Concussion symptoms lasting more that 4 weeks need to be treated as seriously as the concussion itself. Post-concussion syndrome occurs when symptoms last longer than expected after an injury, and can have significant consequences on an athlete’s sport, education and life.
In these cases it can be helpful to see a physio with experience in post-concussion syndrome.
They can address the causes of your symptoms and help you retrain your body and brain to function as optimally as possible.
By Jess Bell
We’d love to hear from you and answer any questions.
Or click through to book an appointment with Jess who has experience in treating post concussion syndrome.
Formotion Physio is a boutique Physiotherapy practice based in Perth, with locations in West Perth, Joondalup & Osborne Park.

Concussion Story: Part 1 - By Jess Bell
Jess talks about her personal experience with concussion and the effects it had on her life. As well as how it was poorly treated initially. She hopes to bring more awareness to this dangerous injury.
Concussion: Part 1 – Jess’ Story
Javelin throwers normally don’t get concussed. It’s a non-contact sport for a reason. But nonetheless in Feb 2020 I find myself lying on the track, head in hands and no clue how I ended up there. Turns out that while I was running down the runway, my spikes got caught together and I fell straight backwards onto my head. And now I was concussed and had no idea what day it was.
I knew I was at the track. And track days were Monday and Thursday.
“Is it Monday or Thursday?” I ask.
“Monday”
“Right, so I’ve got 5 days until the Sydney Track Classic.” Classic Jess – of course the upcoming competition is the first thing on my mind.
We walk to the doctors. With blurry vision and poor balance, I nearly fall in the gutter. I practise saying the months of the year backwards and check my phone to see what the date and time is.
Gotta beat that SCAT-5 test. It’s the sports doctor’s first day at the AIS and he’s completely run off his feet. He says he’s too busy to run through the tests and that I’ll probably be too irritable anyway. We’ll just do it tomorrow.
So I get driven home (a bit disappointed that I practiced my months of the year for nothing) and get left alone to sort myself out. I start vomiting but no one is around to help. Eventually the nausea eases and I get myself into bed, hoping and praying for a miracle when I wake up.
~
The next morning I remember that it’s Tuesday and that there’s a good reason as to why my head is so sore. Sydney Track Classic is only 4 days away. I’m feeling better but the back of my head is still very tender and I can’t string a sentence together.
Sitting in the waiting room, I tell myself that I must pass the SCAT-5 today to prove I can compete on Saturday. The doctor comes out and tells me that I’m looking a lot better. The room spins around me as I say “yes, I know – I’m feeling so good today!”.
My SCAT-5 results are excellent and my months of the year practice pays off. I report that my symptoms are very minor while in reality my eyes struggle to adjust to the bright lights and any movement sends me into a haze. Cleared to return to light cardio, I sit on the bike for 20 minutes before falling in a heap and spending the rest of the day in bed.
The next few days go by and I start to feel more like myself. My SCAT-5 results continue to improve, and the sports doctor dubiously clears me to compete on Saturday after I insist that I will be fine. My reasoning to him – “if there’s even a 1% chance that I can throw well, then I want to give it a crack.”
Great odds when you’ve had a mild traumatic brain injury. Competition day comes around – I fly from Canberra to Sydney as I’m still not allowed to drive. The competition passes in a blur and I throw terribly (surprise).
An absolute mess, I fly home to South Australia to recover and get back on track. My symptoms gradually ease and I start to build some confidence that life can go back to normal.
Wrong.
~
A few weeks later I’m halfway through a throwing session when my vision becomes blurry and I struggle to coordinate my movements. I put it down to having low iron and tell my coach I’d better go chat to the sports doctor to get a blood test.
The sports doctor looks increasingly perplexed as I list off my symptoms. Blurred vision, difficulty concentrating, sensitivity to noise and light, poor balance, difficulty reading and holding conversations. He says “I don’t think you have low iron, I think you have post-concussion syndrome.”
And that’s where the nightmare starts.
I’m told that I have to spend 10 days in a dark room with no mental or physical stimulation. Overwhelmed but with no clue what is going on and whether I even have other options, I do what I’m told. They were probably the longest 10 days of my life. Of course, my symptoms don’t improve – I have difficulty even seeing pitch black properly (don’t ask me how that works).
And so I get sent back for another 7 days of ‘post-concussion recovery’. 17 days in a dark room, right as COVID hits.
Not a good start to 2020.
My symptoms continue and the sports doctor continues to be perplexed. I can’t stay in a dark room my whole life, so I start searching for other options and answers. I’m sent off for a brain scan which comes back normal. The next few months are full of appointments with optometrists, psychologists, neuropsychologists and we have an appointment with a neurologist lined up. I try to do my own research, but there is barely any information on post-concussion syndrome and how to manage it.
It’s easy to wonder whether I’m just making it all up and if there’s even anything wrong with me. All the while, I can barely read a sentence, hold a conversation or focus my eyes. Uni study has to be completed 10 minutes at a time, and I withdraw further and further into myself as my symptoms make socialising almost impossible.
But thankfully, that’s not where the story ends. In one last ditch effort, my Mum tells me to go to a specialist concussion Physio and see if they can help. I didn’t even know Physios dealt with concussions. Doubtful, I walk into the consulting rooms and told the Physio my story. To my immense surprise and relief, he tells me straight out that these symptoms were incredibly normal following concussion and that they can absolutely be managed. A huge weight drops off my shoulders - here was someone who not only knew why I was getting symptoms, but also knew how to manage them.
~
And so the recovery journey began. Despite setback after setback, we worked tirelessly over the next 12 months to manage my symptoms and help me get back to myself again. I can’t say that I’m fully ‘fixed’ or that I never experience post-concussion symptoms anymore. But life is a lot easier now that I can hold a conversation or sit at my desk for longer than 10 minutes.
And as I started to see progress and learn more about concussion management, I swore that I would do everything in my power to ensure that others can avoid being in my situation. Concussion is so easily ignored or dismissed as a minor injury. And so if I can bring even a small amount of awareness to the subject and help one person feel heard in their concussion recovery, then I hope I have done my job.
Now that’s enough dribbling on. This isn’t a story to ask for sympathy, but instead to bring awareness to the fact that concussion is not just a head knock, and that it has lasting impacts in all spheres of life. However with the right help and management, the effects of concussion can be minimised and it is possible for athletes to return to full function.
With a growing base of evidence and more awareness being raised around the topic, we can have hope that spending 2 weeks in a dark room is now a thing of the past.
In Part 2 of this blog, we will look at how concussion SHOULD be managed and strategies for recovering from post-concussion symptoms if they arise.
By Jess Bell
We’d love to hear from you and answer any questions.
Or click through to book an appointment with Jess who has experience in treating post concussion syndrome.
Formotion Physio is a boutique Physiotherapy practice based in Perth, with locations in West Perth, Joondalup & Osborne Park.

Injury Management in Sport
In sport the middle of preseason is often when loads are high, the fatigue is starting to set in and niggles are raising their heads. Unfortunately, pre-season niggles can escalate to in-season injuries if they are not managed appropriately.
The 3 phases of injury management in sport are: Early identification = early management = reduced injury risk.
It’s now the end of February and most winter sports athletes are smack bang in the middle of preseason. Loads are high, the fatigue is starting to set in and niggles are raising their heads.
Some athletes will ignore these niggles and push on without giving them a second thought. Anyhow, who needs two functioning hamstrings to get through a footy season? Unfortunately, pre-season niggles can escalate to in-season injuries if they are not managed appropriately.
So how do we manage these niggles and create the best possible environment for all the preseason work to pay off?
It’s critical to understand the three stages of injury management and strive towards identifying and managing potential issues before they raise their heads.
Early identification = early management = reduced injury risk.
THE 3 PHASES OF INJURY MANAGEMENT

Primary
The primary phase involves identifying and managing potential risk factors to injury before they even occur.
For example, a junior basketballer is about to start ATAR exams and has 2 games of basketball on the weekend. Their S&C coach identifies multiple risk factors:
· The athlete is likely to be sitting at a desk studying for sustained periods. This can lead to hip flexor tightness, neck and back pain, and reduced activity levels
· The athlete is likely to be sleeping less and recovery strategies are not optimal
· Stress levels will be higher than usual, and the athlete may not be as focused during training and games
All of these factors can lead to increased injury risk. If the coach can identify these risk factors early, they can modify their program to incorporate more hip and back mobility, emphasise the importance of recovery, and regularly check in on the athlete. Loads don’t necessarily have to change, but a greater level of awareness goes a long way.
Senior athletes have more self-awareness and should be thinking of these primary management strategies themselves. It’s important that athletes develop a good read of their own bodies and how they respond to different loads and stresses, both physically and mentally. By reporting potential risks to their coach/physio/support team, athletes can help mitigate any concerns before they even arise.
Secondary
Most athletes in preseason will be in this secondary phase where niggles are setting in and fatigue is high. When athletes move into this ‘risk factor territory,’ it’s critical to implement monitoring and management strategies as early as possible. Good athletes will address these niggles and invest in the time to get things right now rather than wait for them to deteriorate.
Secondary management includes:
1. Appropriate recovery strategies
2. Self-monitoring and screening
3. Physio and health practitioner support
4. Modifying loads if needed
Your coaches and physios play a key role in helping athletes through this secondary phase. Physios are not just there to fix your pain and manage your injuries – they’re also there to help you perform at your best and be a sounding board as you build an understanding of your own body and how it responds to load. Leaning on the support team around you in this phase is crucial, and it’s important to maintain communication with your physios and coaches to ensure they can jump on any niggles as soon as possible.
Tertiary
Unfortunately even with the best management and programming, athletes still get injured. There is no bulletproof strategy of injury prevention, and sometimes people just have pure bad luck. However, injuries themselves can be used to learn and grow, and potentially can help athletes and their support staff build a greater understanding of how to approach future situations.
It’s easy to look back and ask what went wrong when an athlete does get injured. But I encourage everyone to also reflect on the injuries that could have arisen, but didn’t, due to early identification and intervention.
By Jess Bell
Physiotherapist

NDIS: Why disability made me a Physio
Some words from our Physio Jess on her personal experience with disability, Physiotherapy and the NDIS.
As we move further into the NDIS and disability space, I asked Jess to share a few words about her personal experience with disability, Physiotherapy and the NDIS.
She came back with some very beautiful and moving words which I would love for you to read!
Why disability made me a Physio - By Jess Bell.
My sister is the main reason that I am a Physio.
She was born with hydrocephalus, an incurable congenital brain
condition that leaves her with many difficulties in all spheres of
life. The only thing preventing her from certain death is a
plastic tube spanning from her brain to her stomach. And it
could block at any time.
If you met my sister today, you wouldn’t even realise she had a
disability. She walks, talks and lives life with an insane amount
of determination and joy. But when you delve deeper, the pain
and struggles she has to overcome to appear ‘normal’ would
blow you away and bring you to tears.
If we take just the past 2 years, she has survived 8 brain
surgeries and still lives with excruciating pain every day. Her
brain literally starts to expand or collapse on itself as it cannot
manage changes in fluid pressure. Trips to the emergency
department are treated like trips to the shopping centre and to
top it off there is the despair of knowing that she may live the
rest of her life with no cure or relief.
Sounds pretty depressing. In some ways it is.
But despite the darkness, there have been some beautiful
things that have come from my sister’s condition.
My sister defied the odds in every way. Much of it was because
of Mum. She was told her daughter would never walk or run. So
Mum bundled us up every week to the physio where my sister
would build her strength, balance and confidence. I would
watch or join in as she attended class after class with other kids
just like her. Hands tightly gripping onto Mum or Dad, she
would spend hours bouncing on the trampoline to build her leg
strength. Holding onto her makeshift trolley, she would
tentatively wobble from one end of the room to the other.
Now, hands tightly grip the reins as she turns her horse to the
next jump. Every week, she walks herself to the general store to get the newspaper so we can do the Saturday quiz together. She runs through life without a single question of whether she is strong enough, balanced enough, able enough.
That’s why my sister is the main reason that I am a physio.
After all those hours watching Physios tirelessly join Mum in her
determination to not let disability beat my sister, I knew that I
wanted to do that too.
Over 4.4 million Australians have a story just like my sister’s. Whether it’s cerebral palsy or autism, acquired brain injury or a congenital condition, each person deserves to have their story heard and to be appreciated for who they are. That’s where the NDIS comes in.
NDIS didn’t even exist until my sister was 13, but the support
and freedom that it gave her and my parents was a godsend. It
now allows her to access regular physio, hydrotherapy and
equine therapy so she can achieve her goals.
Our mission at Formotion is to continue this legacy by helping clients find joy through movement and reach their goals through exercise and hands-on treatment. Physio definitely isn’t the answer to all the challenges of disability, but it can play a major role in building clients’ confidence, strength and function.
Every step toward those elusive goals matters, and it is an honour to join you in the journey.
Jess will be taking on new NDIS clients primarily from our Joondalup clinic which is best suited to kids and teens with disability, however we can also see you from our West Perth or Osborne Park if this suits you more.
For more info please visit our webpage.

3 Ways Exercise Heals Injuries and Improves Pain
The reasons behind why your Physiotherapist makes you exercise when you’re injured.

If you’re reading this we’ll assume that you’ve probably experienced an injury at some stage in your life. You might already have seen a Physiotherapist and possibly been a bit surprised when they gave you exercises to treat it? You may have wondered how exercise would make it better? Maybe you thought things like rest, ultrasound, bandages, surgeries or massage would be the recommended treatment?
In some cases those things are required, but in a lot of cases of musculoskeletal injuries, (those which concern the muscles, tendons, ligaments bones and nerves) exercise is one of the most effective forms of treatment.
For this blog we’ll describe injuries with regard to the 2 major ways they are experienced by you:
Loss of strength/movement/function
Pain
There are countless ways in which exercise improves the healing process, but for now we’ll describe the 3 ways that most directly impact these two “experiences”.
1. Exercise guides your body’s natural healing process.
An acute injury can be described as one that comes on suddenly and often after an obvious “event” where you weren’t injured one minute, and then you were. Like a trip and fall onto your outstretched hand or that sudden “pull” in your calf as you lunged to get that epic tennis backhand.
This is where the demand on the body very suddenly and excessively outweighed what your body could handle and the tissue was damaged in some way. Depending on the severity or complexity of the injury your body has a relatively straightforward plan for healing this kind of thing.
Healing Phases
The first phase is mostly to do with damage control - like clotting any bleeds, sending in more blood vessels, fluid and cells to get rid of damaged tissue and bacteria.
Usually, it also includes a bit of pain to stop you doing any further damage! After this initial phase, “building materials” - like proteins and connective tissues are sent in and set up to begin “rebuilding” the injured site. Together these processes can last several weeks, and usually require a degree of relative - rarely complete - rest to allow your body to do its natural healing thing However this usually overlaps with something called the “Maturation” or “Remodelling” phase where guided exercise, movement and strengthening is so important!
How does exercise help?
The pattern of how your body heals and develops is ingrained somewhat into your DNA, but this acts mostly as a guide (like the blueprint of a house), and your body will only supply what there is a demand for.
So, you need to let it know how much you’ll be “demanding” with regard to how much tissue capacity you need, which you can think of as strength or fitness. During the remodelling phase, the kind of forces, like exercise or movement, you apply directs how and how much of the new tissue - like bone cells, muscle cells/fibres or tendon collagen - is laid down. Bones need pressure to stimulate a strong organisation of bone cells. Muscles and tendons need tension and load to be applied to encourage the cells/fibres to grow in a particular way to be able to do things like contract, stretch or resist tension properly.

Now this doesn’t mean you’re going to wait a week and suddenly go and run a marathon to stimulate your calf tear into healing strongly. This would be creating a sudden demand that far outweighs the current capacity of the still-weak tissue, and can break things down again.
The level of stimulation over time (demand) needs to be at the level, or at least only a little bit more, than the current level of capacity of your injured tissues as well as the recovery capacity, which includes supply of your bodily raw materials (like proteins, fluid, biochemicals, hormones etc) and time necessary for the healing processes to happen. Certain tissues, like tendons and ligaments need a longer time to heal and remodel than muscles or skin.
If you don’t allow for these things you can end up with either not enough, or the wrong kind of cells in a disorganised formation (like scar tissue) which creates poorer quality tissue that is weaker, or less functional, than you would like.
In summary, like all exercise programs, an injury rehab program is one that progresses slowly, where the supply is able to match or catch up to the demand and with enough recovery time or rest to allow periods of adaptation after the stimulus (exercise) is applied.
This is where an experienced Physiotherapist comes in handy to help you find that balance!
2. Exercise takes the stress off the healing part by strengthening the areas around it.
Chronic overuse injuries are ones where the demand has gradually outweighed the supply or ability of the injured part a smaller amount, but over a longer period of time. These injuries usually creep up on you slowly in terms of pain/niggles, and often affect tissues that don’t adapt very quickly - like your tendons. You might not notice the loss of strength/function as much, especially in the beginning. For example, in contrast to the earlier Nadal inspired backhand resulting in the sudden calf “pull/strain”, this would be experienced more as a gradually worsening pain in your achilles, after you made a New years resolution to start playing 4x week - after doing no exercise for the 3 months prior - resulting in our ever common “Too much too soon” explanation for why an injury happened!
How does exercise help?
There are actually 2 ways we can look at this kind of injury:
The affected area itself is too weak or tight for the activity and becomes overloaded/injured.
The structures, like muscles, tendons or ligaments, that should normally support or help out in that activity are weak or tight or the whole system is uncoordinated and that tendon/muscle is having to do all the work and so becomes overloaded.
Often it’s a bit of both, but this is where a specific assessment to figure out which one it is is important so you don’t end up overloading an already overloaded tendon/muscle.

From there you can see how exercise can help - either by strengthening the injured area (see point 1) so it can handle the things you want it to do. Or by strengthening its muscly friends and teaching them how to work together, so the injured bit can get a bit of help to keep up with the demand.
This idea would also apply in instances where a tissue is potentially unable to heal naturally, like in some full thickness tendon/ligament tears where surgery may be an option. Often in these cases strengthening the surround or supporting structures to the point that it can compensate well enough for the damaged tissue is an option - like in a complete biceps tendon tear, which is often not surgically fixed if the patient isn’t bothered by the aesthetic of it!
3. Exercise reduces pain and sensitivity

Pain is probably the most complex part of this list, and we are continually learning more about it.
Pain can be thought of as our body’s “alarm system”. It is a complex combination of nerves detecting things, and your brain deciding if the things are dangerous or not (danger will normally be experienced as “pain” for you).
When you have been acutely injured, or chronically injured, your nerves and brain become super alert to things being dangerous, like movements, touch or even thoughts - particularly ones that are similar to what caused the initial injury. Usually this is a good thing and is designed to keep us safe, and the alarm quietens down as the injury heals, you get stronger and the risk of further injury/danger goes away.
But, in some cases, like if the initial injury was quite severe or traumatic, or lingered for a while, this alarm can become overly sensitive to smaller things that might not actually pose any real danger - like the smoke alarm in your house that is annoyingly set off by the steam of a hot shower!
This also helps to explain how things can be painful but not necessarily injured or have damaged tissue in the way we might expect.
How does exercise help?
Exercise can be used as graded exposure that slowly returns the body to the movements or activities that are painful. Normally the pain settles automatically over time with the increasing sense of safety as the tissue heals and/or you get generally stronger.
In more complex cases like chronic pain, a specifically designed exercise program that takes into account the complex and delicate interaction of your body, nervous system and mental and emotional state is necessary to desensitise things.
There is also growing evidence that cardiovascular exercise acts as a natural painkiller by improving mood through endorphin release as well as increasing blood flow to all areas of the body which can help with healing, as well as nutrient and oxygen delivery to areas of the body.
The body is rather amazing in its abilities to heal, or at least compensate for parts that can no longer do what they’re meant to. Hopefully this gives you some more confidence in your own ability to heal, and will empower you to take action when dealing with injuries!
As Physiotherapists, our role is to guide you through this process.
Movement is Medicine
〰️
Movement is Medicine 〰️
If you would like some guidance on exercise rehab for your injuries please get in touch or book an appointment.
Formotion Physio is a Physio practice located in West Perth, Joondalup and Osborne Park.

Is it DOMS or an injury?
How to tell the difference between DOMS (post exercise soreness) vs Injury, and what to do about both.

How to tell the difference between normal post exercise soreness (DOMS), and injury, and what you can do about both.
DOMS (Delayed onset muscle soreness) is the normal muscle achiness you get after starting an unfamiliar exercise, coming back to training after time off, or after a particularly heavy or high rep training session.
At a microscopic level it is tiny tears of the muscle fibres which is the necessary evil (depending how you look at it!) to stimulate your body to adapt and come back stronger/fitter once the muscle has repaired.
If you’ve never felt it before, or sometimes after a particularly intense session, the discomfort can be so intense that you might start to worry that you might have done something else this time!
We’ve got you covered! Read through the checklists below for the difference between the common DOMS symptoms vs Injury and what you can do about both.
DOMS
TIME FRAME: Usually occurs ~12-24 hours after unfamiliar or intense training, begins to ease after ~48-72 hours. DOMS straight after training often feels more like “jelly-legs” that can still function but are not painful.
WARMS UP: The soreness should ease with continued movement or a warm shower.
LOCALISED PAIN: You’ll be able to find it by pressing the muscle group or area of your body that you trained (e.g. quads if you did squats, lats if you did pull ups). Usually the pain will be about equal on both sides of your body if you trained both sides.
MUSCULAR ACHE WITH USE: No pain at rest - you shouldn’t feel DOMS unless you are using the affected muscle group.
SORENESS WITH STRETCH: Usually you will feel DOMS in the movement direction that stretches that muscle - eg: straightening your elbows with bicep DOMS, walking down stairs with quad DOMS.
WEAKNESS OR ”JELLY ARMS/LEGS”: You might feel like your limbs give way with similar movement patterns as above (we call this eccentric movements), this might improve with warming up.
What you can do about it:
1. Keep moving! Generally DOMS warms up, so once you’re up and going or moving the area it should ease a little. A warm shower can help ease the symptoms too.
2. Wait it out. Don’t worry - it should start to ease up after about the 48 hour mark.
3. Don’t take anti-inflammatories. The inflammation associated with DOMS is a necessary process in adapting and getting stronger/fitter after the training session. Reducing this process can reduce the effect of all your hard work.
4. Don’t over stretch, not to ease the symptoms anyway, it won’t do a whole lot to speed up the recovery so you’re better off just using the time to move gently!
5. Gentle massage might help ease the symptoms slightly for a little while, but it won’t really speed up the process either.
5. Train gently, but don’t go too hard on the same area or with a similar workout, give your body time to adapt or you may end up overloading yourself and in the injury section.
INJURY
TIME FRAME: More severe pain felt during/soon after your training session, or 1-2 hours later once you cool down and doesn't begin to ease naturally. If it worsens after ~48-72 hours it is unlikely to be DOMS.
MIGHT NOT WARM UP: Some injuries won't improve or will worsen with continued movement/use of the painful part. Be careful as some tendon/muscle injuries or strains will also warm up, but then are likely to feel worse once cooled down.
WHERE IS IT: One side notably worse, or pain felt further up or down from the area is likely to not be DOMS. Pain that doesn’t feel like it’s in the muscle, or if it’s very obviously in the joints or tendons is also not normal DOMS symptoms.
TYPE of PAIN: Burning/shooting or sharp, deep throbbing pain at rest, or when the muscle is unloaded is not a DOMS symptom. Catchy, pinchy or clicky pains are also not typical of DOMS.
OTHER SYMPTOMS/NIGHT PAIN: Pins and needles/numbness, and severe resting/night pain that keeps you awake is not typical of DOMS.
WEAKNESS: More severe weakness in a concentric pattern (opposite direction to the muscle stretching), that has no associated pain is less typical of DOMS.
What you can do about it:
If your symptoms are mild you can try to wait-and-see for a few more days and just keep the area moving gently to give the area time to heal on its own.
If the niggling lasts longer than about 4-5 days after the training session in question, it may be worth getting it checked out.
For any severe symptoms, pins and needles/numbness or shooting pain, painful clicking and locking, or simply if you are worried its best to go and see your Physiotherapist or another health professional.
Check out our blog on managing Acute Injuries with “PEACE & LOVE”
Often when we catch and manage injuries early they are easy to manage and you’ll reduce your time off in the long run!
We’d love to hear from you and answer any questions if you are concerned. Or click through to book an appointment.
Formotion Physio is a boutique Physiotherapy practice based in West Perth , Joondalup & Osborne Park, Western Australia

Managing Acute Injuries with PEACE & LOVE
When you've had a sudden acute injury, like a knock, strain or sprain, we now use the acronyms PEACE and LOVE which replaces the previously used RICE to manage it.

For years we have all come to know the acronym “RICE” when it comes to managing an acute injury like a knock, sprain or strain.
With new research this advice has been recently updated, particularly with advice to avoid anti-inflammatories and ice. It also accounts for the higher complexity that often comes with the treatment of injuries throughout their stages to allow them to heal and return to their previous level of strength, or higher!
Instead we now use the two acronyms “PEACE” and “LOVE” which we use for acute (0-4 days) and subacute (4-14 days) respectively. We summarise this below and have included a PDF version for you to keep for future reference which you can download here.
PEACE
When you've had a sudden acute injury, like a knock, strain or sprain, we now use the acronym "PEACE" which replaces the previously used "RICE" to manage it.
P - Protect
Unload the injured part and avoid activities or movements that cause excessive pain during the first few (1-3) days after injury. This is to reduce the risk of bleeding and re-injury. Gentle, pain free movement without loading is generally ok.
E - Elevate
Elevate the injured limb higher than the heart. Elevation can reduce excessive swelling and promotes fluid flow out of he injured tissue.
A - Avoid anti-inflammatory modalities
Anti-inflammatories and can disrupt healing in the acute phase. Blood flow and inflammation drive the healing response and anti-inflammatories in particular can reduce this. The use of ice is also questionable, it can be helpful in reducing pain, however it should be used with caution as it may also disrupt the normal healing processes.
C - Compression
Compress injuries with elastic bandage or tape to help reduce excessive swelling and fluid build up, manage pain and improve circulation.
E - Education
Education is key! It’s important that you understand what is happening within your body and tissues during the healing process, and how an active approach to recovery, rather than a passive approach, can benefit. You'll need to have realistic expectations about what to expect and recovery times.
LOVE
Once your acute injury has settled down after the first few days, we then progress to "LOVE".
L - Load
Loading and mechanical stress promotes repair of your tissues and builds the capacity of muscles, tendons and ligaments. After a brief period of relative rest you need to return to gradual load as soon as possible, guided by pain and your individual advice.
O - Optimism
High levels of concern or stress can heighten sensitivity and cause us to adopt unhelpful coping strategies - such as avoiding movement. Know that your bodies are adaptable, focus on what you can do, plan out how to get back to what you want to do and celebrate progress.
V - Vascularisation
More research is needed on specific dosage, but pain free cardiovascular activity boosts motivation and improves blood flow to the area which can help with healing and recovery. Aerobic exercise is also a natural pain killer so can reduce the need for pain medication.
E - Exercise
Exercise helps to restore mobility, proprioception and strength, particularly specific and progressive exercise. It will also helps to reduce the risk of injuries reoccurring. Return to exercise and training as guided by your pain and any individual advice you have been given.
References
Dubois B, Esculier J. Soft-tissue injuries simply need PEACE and LOVE. British Journal of Sports Medicine 2020;54:72-73.
PEACE & LOVE
•
PEACE & LOVE •
Your individual needs will differ and we always recommend an individual assessment to discern this.
Formotion Physio is a Physiotherapy practice based in West Perth, Joondalup & Osborne Park, Western Australia and we are available for individual appointments.

How to talk to your clients about women's health issues
Personal trainers and coaches are in a unique position where they can screen the general population and the athletes they work with for issues that they may otherwise not feel comfortable bringing up, or not even know that there are solutions to in the first place.
For personal trainers, coaches and fitness professional.
Women’s health issues are very common, but sadly there is not much awareness around it which leaves huge gaps in potential not only for health and quality of life, but also performance.
Women’s Health Physiotherapists and other health professionals who specialise in this area will often only see people when the symptoms have become very extreme.
Personal trainers and coaches are in a unique position where they can screen the general population and the athletes they work with for women’s health issues that they may otherwise not feel comfortable bringing up, or not know that there are solutions to in the first place!
We know that it can be pretty daunting and uncomfortable talking about these issues, especially for men.
Some advice we can give on this is to try and include regular general discussions about it in all of your sessions. Many women may feel embarrassed to raise these issues themselves which is why it’s important to not make it taboo by discussing it regularly, so they know that whatever they are experiencing is nothing to be embarrassed about.
Upskilling in this area will also help you to feel more confident talking about it, see the end of this blog for some links to great resources.
If you don't feel comfortable talking about it, putting a few of the questions below into your initial screening can alert you to refer on if necessary.
Women’s Health Questions to ask:
1. Do you ever experience leakage, or feel like you may leak, during things like heavy lifting, skipping, sneezing or coughing?
Answering yes to this could indicate Stress Urinary Incontinence.
2. Do you ever experience the feeling of pressure in your pelvis/pelvic floor during during things like heavy lifting, skipping, sneezing or coughing
Answering yes to this could indicate symptoms of prolapse.
3. Has your menstrual cycle been normal the past couple of months? (Assuming client is not pregnant or on hormonal contraceptive).
Changes to menstrual cycles can alert you to signs of RED-S in athletes or people that train intensely.
4. How does your cycle affect your mood/energy levels?
Understanding your client’s individual responses to their cycle can help you to plan sessions around this to help them perform at their best.
What to do if your client is having issues?
Considering the pelvic floor and menstrual cycle during training is important, but if your client is having issues they will often need a health professional to diagnoses and treat, at least initially.
Normally these health professionals will aim to work with you and your client to get them back to training with confidence.
At Formotion Physio we have an interest in Women’s Health, and are able to assist with returning to exercise with consideration of the pelvic floor, but we would recommend referring to a Women’s Health Physiotherapist for pelvic floor issues first.
For menstrual cycle or hormonal issues we would recommend referring to a Women’s Health GP or Sports Medicine Physician, particularly if you suspect RED-S (see below) or other more serious health issues.
You can find directory of Women’s Health Physiotherapists on the Australian Physiotherapy Association - Find Physio page here.
A few resources on the topic that we think are helpful and important are listed below:
Continence Foundation of Australia
Julie Wiebe - Women’s Health Physical Therapist
“Pop Up Lift” Instagram page & Website
Jessie Mundell - Pregnancy and Post Natal Fitness Coach
RED-S Relative Energy Deficiency in Sport
RED-S Clinical Assessment Tool
If you know of anymore to add to this list please get in touch or comment on this blog.

What to do when your back "goes"
What you can do in the first day or two of acute back pain or “when you’ve done your back”.

We've been seeing quite a few episodes of acute back pain in the clinic recently, the kind of back injury that people often talk about as "I bent over to pick up my shoe and my back just went”.
Most of the time they are something like a strain or sprain and nothing too serious in the long run, but they can often hurt like crazy and might make you think that you've done something terrible which can add to the intensity of the pain.
Why does it hurt so much?
The intense pain normally lasts about 3-5 days and is because of the acute inflammatory phase of healing, a process that is designed to cause you pain because it wants you to not keep inuring yourself further (It’s a good thing really!)
However with your back this can be quite debilitating because you’ll realise pretty quickly how many movements you need your back for. We also tend to freak out more when we’ve injured something near our spine.
What to do when it happens
Keeping moving gently, don’t stretch or train heavily.
It’s only very rare that complete rest is the answer. With these injuries we normally recommend gentle movement with deep, slow belly breathing to calm the nervous system.
You can start by lying on your back and gently letting your knees rock side to side, stopping before any intense pain but giving it at least a minute or 2 to settle into the movement. Obviously stop if this exacerbates your pain!
Taping
We find taping can calm down some of the fired up nerves and muscle spasming and make everything feel safe and supported until that inflammatory phase has calmed down.
The taping method below is what we use, which can get you through a day or 2 before coming to see us. You'll need a friend to help and we'd advise against the taping if you have tape allergies or any other concerns.
Disclaimer: This post is not a substitute for individual advice. Please get in touch if you are unsure or have a specific issue that needs addressing.
Formotion Physio is a Physiotherapy practice based in West Perth & Osborne Park, Western Australia

First Aid for Ankle Sprains
Ankle sprains or "rolled ankles" can happen when your joint is accidentally bent too far and the ligaments which hold the bones together are stretched or torn.
The first aid we normally recommend for acute sprains is the POLICE principal, rather than the previously used "RICE".

Ankle sprains or "rolled ankles" can happen when your joint is accidentally bent too far and the ligaments which hold the bones together are stretched or torn.
The first aid we normally recommend for acute sprains is the PEACE principle, rather than the previously used "RICE".
Read more about this in our blog here.
P - Protect
Unload the injured part and avoid activities or movements that cause excessive pain during the first few (1-3) days after injury. Crutches may help!
E - Elevate
Elevate the injured limb higher than the heart to reduce fluid pooling.
A - Avoid anti-inflammatory modalities
Anti-inflammatories and can disrupt healing in the acute phase. Blood flow and inflammation drive the healing response and anti-inflammatories in particular can reduce this. The use of ice is also questionable, it is helpful in reducing pain, however it should be used with caution as it may also disrupt the normal healing processes.
C - Compression
Compress injuries with elastic bandage or tape to help reduce excessive swelling and fluid build up, manage pain and improve circulation.
E - Education
Education is key! It’s important that you understand what is happening within your body and tissues during the healing process, and how an active approach to recovery, rather than a passive approach, can benefit. You'll need to have realistic expectations about what to expect and recovery times.
Should I go to the Emergency Department?
In some cases a trip to the ED may be warranted to make sure there isn't a fracture. Signs of a fracture or more severe injury can be:
Inability to weight bear at all.
Deformity of the bones.
Popping/snapping sound at time of injury.
Severe pain at rest or with light touch.
Bear in mind that the pain in the first 3-4 days of an acute injury can often be quite severe, this is the inflammatory process working to encourage you to protect the injury!
However if you are concerned it may be worth taking a trip to a St John’s Urgent Care (Perth, Western Australia only), for an X-Ray as it can often be a bit quicker than the ED.
Regardless of what you are told we would always recommend getting Physiotherapy input to help optimise the healing process through graded stability and strength exercise to reduce your risk of long term instability issues.
Joondalup • West Perth • Osborne Park •
Joondalup • West Perth • Osborne Park •
Your individual needs will differ and we always recommend an individual assessment to discern this.
Formotion Physio is a Physiotherapy practice based in West Perth, Joondalup & Osborne Park, Western Australia and we are available for individual appointments.

How the Upper Back Can Cause Neck Pain.
Pain in the neck can often be related to a lack of strength and mobility in the upper back (thoracic spine).

Pain in the neck can often be related to a lack of strength and mobility in the upper back (thoracic spine).
The Mobility Perspective
When there is a lack of movement in the back, the relatively more mobile joints in the neck often have to compensate in everyday movements which can overload or irritate them over time.
For example, in normal neck rotation the top 4 vertebral bones of the upper back also need to rotate a small amount to allow full range of movement, without this synergistic movement the neck can often feel “blocked” or “catchy”, with pain sometime occurring in the upper back as well.
The “Motor Control” or Strength Perspective
When there is weakness in the upper back there can be an overload or seizing up of the muscles around the neck as they attempt to make up for the lack of strength below or protect the neck.
Often those tight and painful upper trap muscles are a result of this. Instead of spending time stretching or releasing them, working on your upper back mobility and strength might be the key to a long term fix!
What can you do?
It’s best to get an assessment with a Physio you can help you first figure out where the problem lies.
But here are two exercises we like to use to improve movement in the upper back which you can start with.
If in doubt, book an appointment!

Bone Stress Injuries
The best way to build strong and healthy bones, that are resilient to stress injuries later in life, is by exposing them to varied loads which encourages them to adapt and become stronger.

Credit: https://www.ncbi.nlm.nih.gov/books/NBK65798/figure/CDR0000378089__273/
Bone stress injuries (BSI) include stress reactions, stress fractures and complete fractures.
A BSI occurs when there is an imbalance between bone resorption (breakdown) and bone formation. This is usually in response to an abrupt increase in training volume and/or intensity.
BSIs occur more frequently in high load sports such as gymnastics, basketball and cross country. They can occur in any bone. The tibia, metatarsals and the pars interarticularis (lumbar spine) are some of the most commons sites.
These injuries are most common at the beginning of a training season or in the lead up to competition (often due to an abrupt increase in training volume/intensity).
These injuries can be very debilitating and require medical, physiotherapy and often nutrition management.
What can you do?
Prevention is always better than cure! One way we can reduce our risk of developing BSIs is to build a strong skeleton as a child.
After puberty the outer size of the bone cannot be increased so it is important to build strong bones as children. Ensure children are exposed to a wide variety of physical activities that encourage things like running around, changes of direction and lifting weights. These sports that put force on the bones which then stimulate them to adapt to these force and become stronger.
Sports like swimming and cycling, while good for other areas of health, do not place added force onto the bones so are generally not adequate for encouraging bone growth.
Early sport specialisation is not recommended. Early specialisation results in a significant increase in overuse injury compared to young athletes who do multiple sports. Keep things general for most children until high-school where they can specialise with less risk.
If you are currently struggling with a BSI we would suggest getting the help of a Physiotherapist who can help you with load management and return to sport.
By Jason Ciccotosto
Physiotherapist & Gymnastics Coach
B.Sc. Physiotherapy
jason@formotionphysio.com
Formotion Physio is a Physiotherapy practice based in West Perth & Osborne Park, Western Australia

Incontinence During Exercise
Leaking during exercise. What causes it, and what you can do about it.
Does the idea of double unders, box jumps or running make you need to rush off to toilet before you start your workout?
If you've ever leaked, or felt like you might during these movements or things like sneezing or laughing, you might have something called Stress Urinary Incontinence (SUI).
SUI is a pelvic floor issue that affects many women (and men!) whether you've had kids or not, and is common in sports that have movements involving jumping/high impact or heavy weights.
While it is common, it does not mean it is normal.
There are exercises and strategies you can learn that can teach your pelvic floor how to function during these more demanding activities.
What is the Pelvic Floor?
The culprit is likely to be the trampoline-like group of muscles at the bottom of your pelvis called the Pelvic Floor.

The pelvic floor is important when it comes to controlling when, and when you don't go to the toilet. It is also important for supporting and keeping all your abdominal and pelvic organs inside you, as well as during sexual function.
If this group of muscles isn't working correctly and the pressure in your abdominal area increases suddenly - for example if you lift heavy/jump/cough/sneeze or bend over quickly, the control and contraction it normally puts around the urethral and anal sphincters to stop you going, can be overcome by the pressure, which can lead to leaking either urine or faeces.
What can you do about it?
Traditional pelvic floor exercises, sometimes known as "kegels", are the ones that are recommended most often. These are the ones where you squeeze as if you're trying not to go to the toilet, and are usually encouraged while you’re relaxing in sitting or standing, like at traffic lights or queue at the checkout.
While these can be a good first step to creating awareness of these muscles, they don’t give you the full picture. This may be why you can you still have problems when it comes to intense exercise and coughing/sneezing, even if you are religiously doing them.
Pelvic floor “weights” have also become quite popular recently, however these also have their limitations (see below).
Make sure you are able to contract, and relax correctly.
It may be that you are weak, the muscles are too tight, or you are not using the muscles correctly.
It is important that you are able to gently “lift” the muscles. The action is the one you would use to stop yourself going to the toilet, you should have awareness and be able to control both the front and back passage. Often people will have more control of one but not the other so it may give the perception of good function, but in reality there is a lack of control where it matters.
The ability to relax when required is also just as important as this allows you to go to the toilet, for sexual function and also to rest the muscles.
A muscle that is always wound up and switched on will eventually become too fatigued to react and work when it is required. They can also cause pain with penetration in some cases.
*This is why pelvic floor “weights”, which you generally walk around with for a long time without getting that all important rest and relax time, are not recommended.
Try it.
1) Lie down or sit in a deep squat if you can.
2) Imagine you are trying to hold in a wee. A cue we love is “Pick up a jelly bean with your vagina”. For men a good cue is “Nuts to guts”. It should just be a small contraction, imagine it is moving about 5mm.
3) Relax and notice if it feels like the pelvic floor is dropping back down.
4) Now try it with your back passage, as if you are trying to hold in wind. Usually this one is easier so make sure you can differentiate between the front and back.
5) Then try and do them both at the same time. Making sure to relax in between.
6) You can build strength by performing a strong or hard contraction, for example a “1cm” lift which you can try to hold for 2-5sec.
7) For endurance try to hold a gentler contraction for a longer; 10-20 seconds for example.
A cue we don’t love is “belly button to spine” because this generally cues the upper abs and can create more downward pressure on the pelvic floor.
Test it.
A quick test you can try is attempting to stop a stream of wee while on the toilet, if you can then you’re likely to be contracting the muscles correctly.
If you can’t, or you end up “pushing down” then this is probably a sign that you lack strength and awareness and you’ll probably need some help from a Women's/Men’s Health Physiotherapist to teach you how to to activate correctly.
Make sure you only do this very occasionally as doing it too often increases your risk of urinary tract infections.
Combine it with functional exercise.
Once you are confident with this then the next step is to make sure your strength and timing is working well during more complex and intense activities.
As we explained before, instead of being constantly contracted, your pelvic floor should be able to respond fairly automatically to these sudden increase in pressure at the right time, and relax when the pressure subsides so that the muscles can rest.
Randomly squeezing and relaxing your pelvic floor, without training towards a functional goal can be likened to just tensing and relaxing your biceps, instead of using them to bend your elbow at the time you need to lift something up.
Functional Example
Gently squeezing and lifting right before you go for a 1RM squat.
Cueing a few “quick squeezes” before you start a round of skipping to get the muscles and nervous system ready for the type of contraction it will need to be doing.
Your body is also designed to work in movement patterns, as opposed to using single specific muscles. When there is a functional goal this cues a movement pattern that can create more force than an isolated contraction. For example your bicep will create more force by climbing up a rope than by simply tensing it as hard as you can. In the same way, your pelvic floor is better engaged during an action that has the context of a useful function.
Consider the big picture of technique.
To give your pelvic floor the best chance of being able to manage extra pressure, make sure the rest of your technique is spot on to put your body in the best position for the pelvic floor to work at its best.
For example if you are “donkey kicking” during your double unders (skipping) the force you are hitting the ground with a lot more, this means that the downward force of your abdominal contents onto your pelvic floor is also a lot more which can overcome even a relatively strong and coordinated pelvic floor.
Your running and lifting technique will also play a big part in this.
Train your pelvic floor like you would any other muscle.
Once your technique has been considered, train in a way that works within your body’s limits.
For example if you are leaking after 20 skips then this is more than your max. Instead try building up your endurance by starting with 3x10 skips and build up from there.
If you feel like you are about to leak with an 80kg squat, then maybe 79kg is your 1RM? Adjust your mindset so that even if you can lift the weight it doesn’t count unless your pelvic floor is able to lift it to.
This is how you’ll keep yourself safe and be able to continue the sport you love in the long run.
Where to from here?
We can only fit so much information in a blog, and this information might not be appropriate for your individual needs.
So as usual we’d suggest getting help from a professional to first help you figure out the reasons it might not be functioning correctly and address these issues first.
Once you’ve done that you can begin learn how to improve your awareness of it and incorporate it into your daily life or training. This is something we can help you with as it is often a lot more complex than what we’ve written here.
If you have any issues related to traumatic childbirth or have severe issues we’d suggest seeing a specialist Women’s Health Physiotherapist. Feel free to contact us for any recommendations.
By Lucia Tennant
Principal Physiotherapist
B.Sc. Physiotherapy
Director - Formotion Physio
lucia@formotionphysio.com
Formotion Physio is a Physiotherapy practice based in West Perth & Osborne Park, Western Australia

3 Running Tips to Improve Overstriding
Overstriding can slow you down and make running feel heavy and painful. If this is something you do try these 3 tips to improve your technique.

Despite what you’d think, running isn’t something everyone naturally does well, and overstriding is probably the most common issue we see in beginners and even our more seasoned runners.
Simply put, overstriding is when your foot stretches out and contacts the ground too far in front of your body when you take a step.
This effectively causes a stopping, breaking action which can also be quite jarring on the body. It tends to make running feel heavy and hard, and is often the culprit of pain in the shins, knees, hips and back during running.
It also means there is extra time needed for your body to get into the right position to then push off for the next stride, which slows the whole process down even more and wastes precious running energy!
See the video below for an example:
3 tips to improve overstriding.
Stride faster, not longer.
A more efficient way to run faster is by taking quicker steps that land close to the body, avoiding the stopping action, and allowing you to be in a better position to push back to propel yourself forwards in the next step.
See the video below for our same client a few months after practising!
To do this you can try focus on these three things next time you run:
Take shorter, quicker steps, rather than striding out
Often we’ll see people striding out to try to pick up their pace, which may sound correct, but usually results in more overstriding.
Aim to land close to your body, more towards the middle of the foot.
While the research tells us that there is nothing wrong with a heel strike, in practice with our clients we find that cues to pull your foot back to land more in the middle to front of the foot can help to achieve this better.
Think about “staying tall” & leaning forward.
Imagine a string pulling you ‘up towards the sky’ as you run, this will keep you extended and stable in your hips and core.
Lean forward slightly with the whole body, as opposed to just bending at the hips. It should feel like you would fall over if you didn’t put your foot out to stop yourself.The faster you go the further forward you should lean (up to a point!)
Staying too upright, especially as you try to pick up the pace, will cause you to reach out too far in front of you again.
If you are having trouble getting your head around these tips, or for advice that is specific to you, book an appointment with us or come along to one of our running technique workshops.

Do you really need to squat so straight?
Why it’s ok for your knees to go over your toes and for your feet to be wider than your hips when you squat.

There are a few old ideas and myths that come up in the clinic, which we often have to spend a good chunk of time re-educating about. A few of which relate to how you should squat.
The two main ones which we’d like to bust with this blog are:
“You should never let your knees go over your toes”
&
“You need to squat with your feet and knees straight forward, or in line with the hips”
⠀⠀
These misconceptions are based on some old research, but as we know, research is continuously being updated and improved on. These ideas have since been found to not be true as a blanket statement.
If you have been told and believe either of these things, this blog is to free you from these ideas and give you permission to move and squat how your body was designed to!
Lets break them down:
Myth 1. “You should never let your knees go over your toes”
⠀
In short, in healthy populations, it is completely fine, and actually good for your knee joints and muscles to move and get stronger throughout their whole range of movement.
⠀
It can also help improve your squat technique by allowing you to distribute your weight better. Without bending your knees enough you have to compensate by either leaning forward or excessively bending the hips to get your full depth squat.
Your body is designed to squat low - think of the movements of a child, almost everyone in Asia, or you, when camping and nature calls! (Possibly not quite as comfortable looking, yet!)
Watch this video to see the difference:⠀
We will say though, if you have been avoiding this for a while, you’ll need to slowly re-introduce it so your knees have time to adapt to moving into a range they are unaccustomed to.
Myth 2. “You need to squat with your feet and knees straight forward, or in line with the hips”
Everyone’s hip joints are a slightly different shape, check out these two femur (thigh) bones to see what we mean!

This means your squat will look different depending on your body’s anatomy.
⠀
Forcing your knees/feet to move straight forward when your body and bones aren’t designed to is often a reason for finding the whole experience difficult, “pinchy in the hips” or uncomfortable, no matter how much mobility work you do!⠀
⠀
Watch this video for the difference in ability to squat to full depth with the feet and knees in line with the hips vs wider than the hips.

In short, the best position is whatever is most comfortable for you, and whatever is best for you to produce force (lift heavy things). ⠀
⠀
We suggest playing with a few variations of foot width/turn out and see what works best for you in terms of comfort/force production. Generally it’s best to pick somewhere in the middle of your ideal range (not too wide/narrow) so you have room to move either in or out if required, or to land slightly wider for our olympic weightlifters.
Please note that if you have been told to squat in a particular way for a specific medical reason, then please carry on with whatever works for you!
Still stuck? Let us help you.
Formotion Physio is a boutique Physiotherapy practice based in West Perth & Osborne Park, Western Australia
By Lucia Tennant
Physiotherapist and Founder of Formotion Physio
BSc Physiotherapy

Can you fix your “flat feet”?
Why orthotics and excessive arch support shouldn’t be forever, and how you can train yourself out of them.

“Flat feet” have become synonymous with something that people have, and aren’t able to change, and so are doomed to wearing orthotics and only shoes with arch support for the rest of their life.
But what we really mean here is, can you naturally fix your weak feet, and the simple answer is most of the time, yes!
What are flat feet?
In simple terms flat feet refers to a low arch of the foot that is unable to support itself and spring back when needed. It is often coupled with over-pronation where there is an excessive amount of “rolling in” of the foot and ankle.
Naturally your foot moves between pronation and supination when walking, running and jumping, just like your knee bends and straightens. While pronation, and the ability of the arch to flatten is a normal and necessary movement, it becomes a problem when it can’t spring back and roll back out when needed.
Your foot spring accounts for around 8-17% of the energy you use in running, think of all that loss of power if it is weak! (Kelly et al. 2018)
The good news is, like every other part of your body, unless you have a fixed structural issue (referring to how your bones are developed), often excessively flat or overpronated feet are caused by a lack of strength and control in your ankle and foot muscles, which is something you can change with exercise training.
Do you need orthotics or shoes with arch support?
When your feet aren’t functioning well it can sometimes cause issues with the foot, or further upstream, like at the ankle, knee or hip. This is often treated with orthotics or supportive shoes which keep the arch of the foot up and block the foot and ankle from rolling in.
These can be good in the short term to take the load off those areas while they heal or get stronger, but they should always be coupled with an exercise program. Orthotics alone don’t strengthen the muscles or train your foot how to move properly, they can actually do the opposite and cause you to be more reliant on the orthotic as well.
Just like you wouldn’t generally wear a back brace forever for a weak back, you shouldn’t brace your foot forever without also training it to function on its own.
What can you do instead?
If you are wearing orthotics make sure you have an active approach (exercises) that go with them - unless you have a specific reason, in most cases you should be aiming to train yourself out of them. The same goes for the heavily arch supported shoes out there.
This doesn’t mean that you should jump straight out of your orthotics and into a minimalist shoe - like any exercise program it should be a slow graded process over a few months.
If you know you have flat, or weak feet and ankles, you can start a graded exercise program to start strengthening them, and consider opting for a slightly less supportive shoe the next time you buy.
Anything that stimulates the ankle and foot muscles and encourages balance, like single leg work with a focus on alignment and things like pressing the big toe into the ground or gripping the ground are a good place to start.
Or simply just go for barefoot walks outside or along the beach!
If you’d like some more info, or if you need specific guidance with this please get in touch, or book and appointment, we’d love to help you!
Formotion Physio is a boutique Physiotherapy practice based in West Perth & Osborne Park, Western Australia
Written by Lucia Tennant
Physiotherapist and Founder of Formotion Physio
BSc Physiotherapy
1) Luke A. Kelly,1 Andrew G. Cresswell,1 and Dominic J. Farris1,2 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6043578/